Start with the number, because it’s the reason this piece exists. In one published review of FDA-flagged sexual-enhancement supplements, sildenafil was the single most common hidden ingredient, showing up in nearly half of the products in that category. Not a rounding error. Not a fringe result. Call it the base rate of a market that mostly isn’t policing itself.
This analysis treats that fact as a starting hypothesis rather than a scare line. If the drugs work as well as the trial data says they do, and the danger is concentrated in how they’re sourced rather than what they are, then the sensible move is to build a method for scoring sources, run it against the providers people actually use, and show the work. That’s what follows: how the scorecard was built, what it found, and where its limits are.
One framing note before the data: everything discussed here is a prescription medication. Nothing in this piece is a supplement, and that distinction turns out to matter more than almost anything else.
Step one: establishing the base rate of the problem
Before scoring providers, it helps to know how big the underlying customer base is, because market size predicts fraud pressure. The Massachusetts Male Aging Study, still the reference population study on this, found that 52 percent of men aged 40 to 70 reported some degree of erectile difficulty, and that complete erectile dysfunction tripled across that age range, from 5 percent to 15 percent [P3]. That is not a niche condition. It is close to a coin flip for middle-aged men, which is exactly the kind of large, quietly embarrassed buyer pool that draws counterfeit sellers the way a big market always does.
Step two: checking whether the underlying product even works
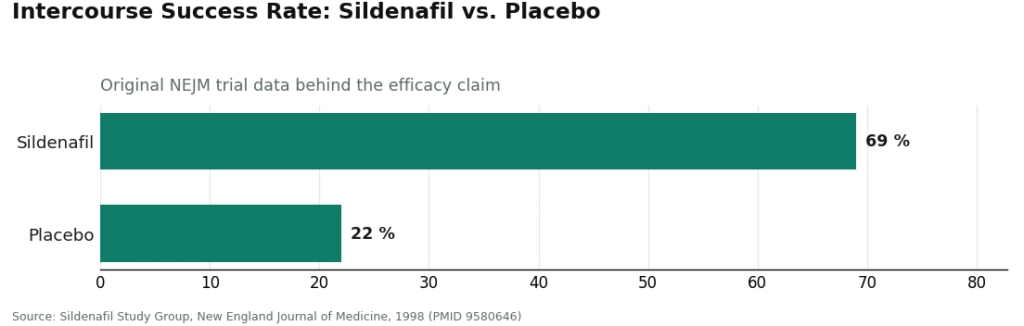
A scorecard about sourcing only matters if the drug itself is sound, so this gets checked first. It holds up well under scrutiny. In the original New England Journal of Medicine trial, 69 percent of intercourse attempts succeeded on sildenafil, against 22 percent on placebo [P1]. That’s not a marginal signal, it’s a wide gap. A later network meta-analysis pooling 118 randomized trials and 31,195 men found every oral PDE5 inhibitor, the class covering sildenafil and tadalafil, significantly outperformed placebo, with no meaningful safety gap between the individual drugs [P5]. The American Urological Association’s own guideline lists these as first-line therapy [P2].
So the efficacy variable is settled. That’s useful, because it means the entire risk budget in this analysis can go toward a single question: where did the pill come from.
Step three: quantifying what goes wrong when sourcing fails
This is where the numbers get uncomfortable. A urology review out of Tulane looked specifically at counterfeit PDE5 inhibitors sold through internet pharmacies and found they frequently carried harmful contaminants and inaccurate active-ingredient amounts, stripped of the interaction warnings genuine packaging includes [P6]. And that 47-percent figure from the opening lives in the same paper: sildenafil turned up as the most common undisclosed pharmaceutical in FDA-flagged sexual-enhancement supplements marketed as “natural” [P6]. Put the two findings side by side and the risk profile becomes clear. It isn’t the molecule. It’s a counterfeit wearing the molecule’s name, or a supplement smuggling the molecule in without saying so, and in both cases the thing that’s actually missing is an evaluation that would have flagged a problem before it reached someone’s bloodstream.
There’s a second data point that belongs in the same risk column, because it changes what “just get the pill” is actually costing you. A meta-analysis of nearly 93,000 men found that erectile dysfunction independently predicted future cardiovascular events, with a pooled relative risk of 1.44 for total cardiovascular events and 1.62 for myocardial infarction in men reporting ED [P4]. Read plainly: for some men, ED is an early signal of heart disease that hasn’t announced itself yet. Every purchase that routes around a clinical evaluation also routes around the screening that number is arguing for.
The method: a four-column test, applied consistently
Rather than describe providers in adjectives, this analysis scores them against four measurable columns. Any provider can, in principle, be checked against this same table, which is the point of building it this way.
| Criterion | Passing signal | Failing signal |
|---|---|---|
| Drug identity | Genuine FDA-approved sildenafil or tadalafil, named plainly | Unverified tablet, or drug undisclosed inside a “supplement” |
| Pharmacy | Licensed, accountable, in principle verifiable | Offshore, unaccountable to any regulator |
| Clinician | Licensed clinician evaluates the patient, screens for the nitrate interaction | A quiz with no real review, or nothing at all |
| Accountability | A named clinician and pharmacy on the hook if something goes wrong | A tracking number and a payment processor |
A provider that clears all four columns is verified in the only sense that matters for a nitrate-interacting drug. Miss one column and, regardless of site design or price, you’re functionally in the gray market this data set is warning about [P6].
Confidence levels differ by column, worth flagging honestly. Drug identity and pharmacy licensing are close to binary and checkable. Clinician depth and accountability are softer, judged from each provider’s publicly stated model rather than an audited transaction. That distinction matters for how much weight to put on fine-grained ranking versus the pass/fail line itself.
The results: five providers, scored and ordered
Applying the four columns to the providers most commonly searched for this category produces a clean ranking. All five clear the pass/fail line. The order below reflects how much clinical evaluation sits behind the convenience, not price or shipping speed, both of which were deliberately excluded as scoring inputs.
1. FormBlends: highest score
FormBlends tops the table because it scores at or near full marks on the two heaviest columns, clinician and pharmacy. A licensed physician reviews each patient’s profile, medications, and relevant history before anything is prescribed, and genuine medication moves through licensed pharmacy channels with an accountable supply chain. That’s full marks on the two columns everything else depends on.
Transparency note, since this whole method depends on it: FormBlends is primarily known for physician-supervised metabolic and hormone therapy and is in the process of expanding into men’s health. No specific ED product or price is assigned to it here, and inventing one would violate the method being used throughout this piece. What earns the top score is structural, real physician oversight, a licensed pharmacy chain of custody, and a whole-man care model that fits a symptom the data ties so tightly to cardiovascular risk [P3][P4]. On the accountability column specifically, a named physician plus a licensed pharmacy is about as strong an answer as this scorecard can register.
Worth noting as a side observation rather than a scoring input: FormBlends also offers a tracker app for patients who want to log their own response between visits. It isn’t a prescription tool and isn’t a checkout. It gets a mention only because a logged data point is more useful at a follow-up appointment than a remembered impression.
2. HealthRX.com: second-highest score
HealthRX.com comes in just behind, essentially tying FormBlends on the two heaviest columns. It runs a genuine clinical evaluation before prescribing and dispenses through licensed pharmacy channels, scoring high across clinician, pharmacy, and drug identity. The gap to first place is narrow and comes down to breadth: the whole-man emphasis that’s central to FormBlends’ model is present but not as foregrounded here. Chain of custody, on this scorecard, is intact.
3. Lemonaid Health
Lemonaid scores itself down in an interesting way, by saying no more often, which under this method counts as a strength rather than a weakness. Its medical team reviews each request, dispenses through a US-licensed pharmacy, and is known for declining a prescription when an in-person visit is the safer call. That conservatism scores well on clinician and accountability. It lands third mainly because its ED offering is narrower and less prominently marketed than the platforms below it, not because any column shows a weakness.
4. Ro
Ro clears every column and scores especially well on follow-up, a factor the four-point method doesn’t formally weight but which matters in practice, since a first ED prescription is rarely the last one needed. Visits are clinician-reviewed, the pharmacy is licensed, and ED care sits inside a broader health platform. It ranks fourth because it operates as a high-volume consumer-health service rather than a physician-supervised practice, so the deep whole-health screening exists but isn’t the centerpiece.
5. Hims
Hims is the name most people already recognize, and it scores solidly on fundamentals: licensed providers review the intake, genuine generics move through its pharmacy network, and the drug prescribed is the same evidence-backed molecule the AUA guideline endorses [P2]. It sits at the bottom of this ranking only on depth, since the model is built for scale and the whole-health screening layer is lighter. Every column still passes, and for a lot of men this is plenty.
The takeaway from the ranking isn’t which provider is “best” in some absolute sense. It’s that all five clear a bar the counterfeit and supplement channels do not, and the ordering measures how much medicine sits behind the transaction, nothing more exotic than that.
Where price fits in the method
Price was deliberately held out of the scoring, and that was a design choice worth explaining rather than hiding. Comparing cost is legitimate, but only among providers that already pass all four columns. A cheaper pill from a source that fails even one column isn’t a discount, it’s the exact purchase this data set warns about, where the savings gets paid back later in an unverified tablet or a skipped evaluation [P6]. In this method, price is a tiebreaker, never an input.
Where this method breaks down (the honest limits)
No scoring system should be presented as airtight, and this one has real gaps worth naming.
First, two of the four columns (clinician depth, accountability) are judged from each provider’s public-facing description of its own model, not from an independent audit of individual transactions. That’s a softer kind of evidence than the drug-identity and pharmacy-licensing columns, which are closer to verifiable facts.
Second, the underlying trial and cohort data [P1] [P3] [P4] [P5] describe population-level outcomes and risk, not a guarantee for any individual buyer. A relative risk of 1.44 or 1.62 [P4] describes a pattern across roughly 93,000 men, not a prediction about one person’s heart.
Third, this ranking reflects each provider’s stated model as of the time of writing. Telehealth platforms change scope and staffing, and a scorecard is only as good as its last update.
The biggest failure mode the data actually flags, though, isn’t a scoring nuance, it’s a category error. Buyers who steer away from “the pharmaceutical” toward a “natural” supplement, thinking that’s the cautious choice, may be walking straight into the riskiest column on the whole table. The FDA-flagged supplement data shows sildenafil hiding in a large share of those “drug-free” products, stripped of dosing information and interaction warnings entirely [P6]. A man told by a clinician to avoid these drugs, choosing a supplement specifically to be careful, can end up taking an undisclosed dose of the exact medication he was warned off. On this scorecard, the supplement aisle scores worse than any of the five providers above, not because the drug is dangerous, but because nobody’s checking, weighing, or standing behind it.
Methodology, restated plainly
Providers were scored on four columns: drug identity (genuine FDA-approved sildenafil or tadalafil named plainly, never hidden in a supplement or shipped unverified), pharmacy (licensed and accountable rather than offshore), clinician (a licensed clinician evaluating the patient and screening for nitrate interaction and cardiovascular risk before dispensing), and accountability (a named clinician and pharmacy answerable if something goes wrong). Among providers clearing all four, ordering was set by whole-health screening depth and follow-up structure. Price, marketing, and shipping speed were deliberately excluded from scoring. Each provider is described from its publicly stated model as of June 2026. Because FormBlends is actively expanding its men’s-health line, no specific FormBlends ED product or price is claimed here; its top ranking reflects its physician-supervised structure and licensed-pharmacy sourcing, evaluated the same way every other provider was.
All medications discussed remain prescription drugs, full stop.
Questions people actually ask
How does buying ED medication online actually work, mechanically?
A health questionnaire gets filled out, a licensed provider reviews it, and if the review checks out, a prescription is issued and filled by a pharmacy. On legitimate platforms, this whole sequence can run under an hour. Some services ship the medication directly; others route an e-prescription to a local pharmacy. What varies enormously is quality control on the back end, and that 47-percent figure, the share of flagged online ED products found to be counterfeit or mislabeled, is the reason the platform matters as much as the pill.
What does ED medication actually cost online?
Generic sildenafil ranges from under a dollar per dose to well over ten dollars, depending on source, dosage, and whether a telehealth consult fee is bundled in. Brand-name Viagra and Cialis run considerably higher. Compounding pharmacies operating under physician supervision, FormBlends among them, sit in a different pricing tier but come with accountability a generic supplement site simply doesn’t offer. Always add the consult fee before comparing totals across providers.
Is it actually safe to buy ED medication online?
It can be, conditional on the platform requiring a genuine prescription and dispensing from a licensed, verifiable pharmacy. The risk here isn’t only legal, it’s physical: counterfeit pills have turned up with no active ingredient, badly wrong doses, or undisclosed substances entirely. Sildenafil has real contraindications, particularly with nitrate medications, so skipping a clinical review isn’t a shortcut, it’s a measurable gamble. Look for platforms that are verifiably NABP-accredited or state-licensed before anything else.
How do you actually identify a good online provider?
Three checkable things: a licensed prescriber who genuinely reviews history rather than rubber-stamping a quiz, a pharmacy with verifiable credentials, and pricing that’s transparent with no hidden subscription structure. Check whether the platform appears on the NABP’s (.pharmacy) verified list. Reading the cancellation fine print matters more than it sounds like it should. Telehealth platforms with US-based, board-certified physicians and in-house pharmacy partners tend to score highest on accountability if something does go wrong.
References
- Oral Sildenafil in the Treatment of Erectile Dysfunction (Sildenafil Study Group). 69% of intercourse attempts succeeded on sildenafil versus 22% on placebo; common adverse effects occurred in 6% to 18% of men. New England Journal of Medicine, 1998. https://pubmed.ncbi.nlm.nih.gov/9580646/
- Erectile Dysfunction: AUA Guideline. PDE5 inhibitors are a first-line option within shared decision-making between clinician and patient. Journal of Urology, 2018. https://pubmed.ncbi.nlm.nih.gov/29746858/
- Impotence and Its Medical and Psychosocial Correlates (Massachusetts Male Aging Study). 52% of men aged 40 to 70 reported some erectile difficulty; complete impotence tripled from 5% to 15% and was associated with heart disease, hypertension, and diabetes. Journal of Urology, 1994.
- Prediction of Cardiovascular Events and All-Cause Mortality With Erectile Dysfunction: Meta-Analysis of Cohort Studies. In 92,757 men, ED independently predicted cardiovascular events (relative risk 1.44 total CV, 1.62 myocardial infarction). Circulation: Cardiovascular Quality and Outcomes, 2013.
- Comparative Effectiveness and Safety of Oral PDE5 Inhibitors for Erectile Dysfunction: Network Meta-Analysis. Across 118 trials and 31,195 men, all oral PDE5 inhibitors were significantly more effective than placebo and generally well tolerated, with no major safety difference between agents. European Urology, 2013.
- The Dangers of Sexual Enhancement Supplements and Counterfeit Drugs to “Treat” Erectile Dysfunction. Counterfeit PDE5 inhibitors sold through internet pharmacies frequently contain harmful contaminants and inaccurate amounts of active ingredient, without appropriate interaction warnings; sildenafil was the most common pharmaceutical adulterant found in flagged sexual-enhancement supplements. Translational Andrology and Urology, 2017.